

Abstract
Introduction
Extracorporeal membrane oxygenation (ECMO) is a life saving measure for severe respiratory (veno-venous ECMO [VV-ECMO]) or cardiac (veno-arterial ECMO [VA-ECMO]) failure. Heparin induced thrombocytopenia (HIT) is a special concern in these patients because ECMO uses a modified cardiopulmonary bypass (CPB) resulting in continuous exposure to artificial surfaces and unfractionated heparin (UFH) over several days to weeks, compared to CPB in which these exposures are for only a few hours. In addition, most of the patients undergoing CPB do not have underlying systemic inflammation and have a normal platelet count at the time of first exposure to UFH. It is possible that patients receiving ECMO are at higher risk of developing HIT compared to patients having CPB. The prevalence of HIT in adult patients receiving VV-ECMO is unknown.
We determined to ascertain the incidence of thrombocytopenia and the reliability of pre-test probability score (PTPS) in predicting HIT, in patients receiving VV-ECMO or VA-ECMO compared to CPB. Differences in the PTPS of patients on ECMO compared to patients who received CPB and the effect of HIT on 30-day mortality in ECMO patients compared to patients who did not have HIT were also assessed.
Methods
This was a single centre retrospective study of patients undergoing CPB (median 4.6 [2-16.5] hrs. or receiving ECMO for ≥ 48hrs (median 7.1 [3-42] days. HIT screening was performed in all patients who showed a typical pattern of platelet drop in first 5 to 12 days after exposure to UFH with or without thrombosis. A citrated blood sample and a completed PTPS (4Ts) were collected from all patients prior to a screening test for HIT antibody performed on an ACL TOP500 analyser using Hemosil HIT-Ab (PF4-H) kit (Werfen UK). Those with positive HIT screening had confirmatory testing by ELISA (HYPHEN BioMed, France). Clinical data were collected from electronic records. From January 2016 to April 2018, 296 ECMO patients (142 VA-ECMO, 156 VV-ECMO) and 2998 CPB patients were studied.
Results
CPB patients were older than the patients who received ECMO; mean age (standard deviation) for EMCO and CPB were 45.4 (±15.6) and 64.9 (±13), p< 0.00001. A significantly higher proportion of men had CPB (71.3%) and ECMO (58.5%) than women, P<0.0001.
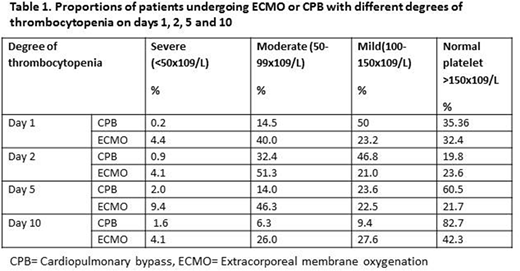
Thrombocytopenia was divided into mild (platelet count 100-150x109/L), moderate (50-99x109/L) and severe (<50x109/L)). Table 1 demonstrates the percentages of patients in ECMO and CPB with different degrees of thrombocytopenia on day 1, 2, 5 and 10. The incidences of severe thrombocytopenia and moderate thrombocytopenia were 4.4% and 40% already on the first day of ECMO which were significantly higher than in patients having CPB (p<0.0001) and this difference remained significant in day 2, 5 and 10. The proportion of CPB patients with moderate thrombocytopenia rose to 32.4% on day 2 from 14.5% on day 1 but by day 10 platelet count was normal in 83% compared to 42.3 % patients receiving ECMO.
A total of 96 patients had HIT screening tests (64/296 ECMO and 32/2988 CPB). Twenty patients (20/296, 6.8%) on ECMO (11/142, 7.7% VA-ECMO and 9/156, 5.8% VV-ECMO) had a positive screening test compared to 18 patients (18/2998, 0.6%) on CPB (p<0.001). All positive screening tests were confirmed by ELISA (100% positive predictive value). The median PTPS for patients on ECMO was 4 (3-7) whilst for patients who received CPB it was 5 (4-7). Four ECMO patients had PTPS of 3 and would not normally been screened according current guidelines. All patients with confirmed HIT were treated with argatroban. There was no difference in mortality between ECMO patients who did or did not developed HIT; overall mortality: 95/296, 32.1%, mortality in patients without HIT: 89/276, 32.2% and patients with HIT 6/20, 30%)
In conclusion, severe and moderate thrombocytopenia is already common in patients receiving ECMO on the day of the ECMO initiation. Patients who had CPB dropped their platelet count to mild to moderate levels on day 2 and 5 and then recovered by day 10. HIT is more frequent in patients receiving ECMO (both VV and VA-ECMO) compared to patients who had CPB. Although the PTPS was good at predicting HIT in patients who had CPB, it failed to detect HIT in 4/20 (20%) ECMO patients.
Jayakody Arachchillage:Bayer: Other: Sponsored to attend educational meetings; Octapharma: Other: Sponsored to attend an educational meeting; Mitsubishi Phama: Other: Sponsored to attend an educational meeting. Laffan:Roche: Consultancy, Speakers Bureau; Pfizer: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal